🌍✨ Celebrating Our Calabar Cohort ✨🌍
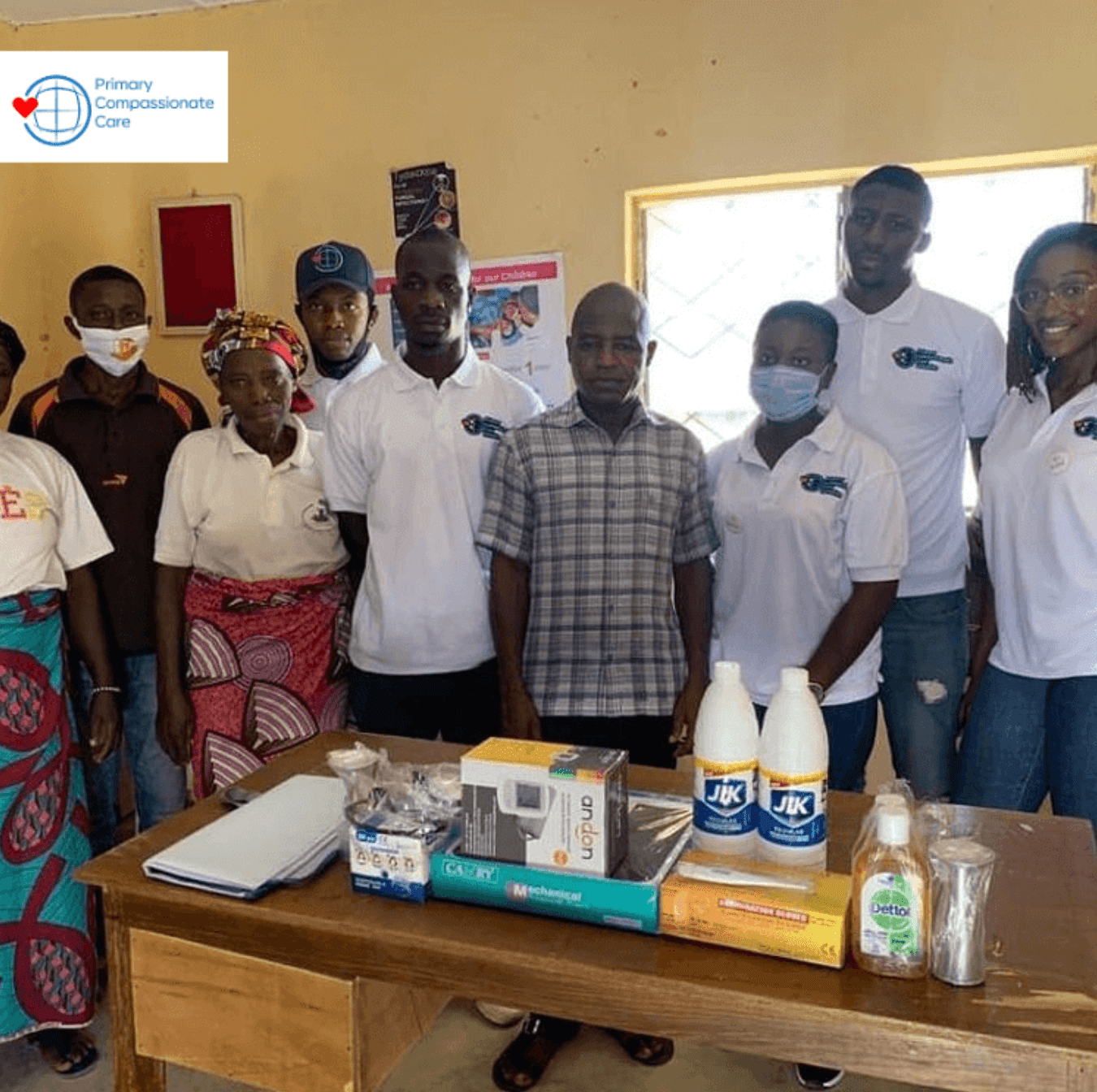
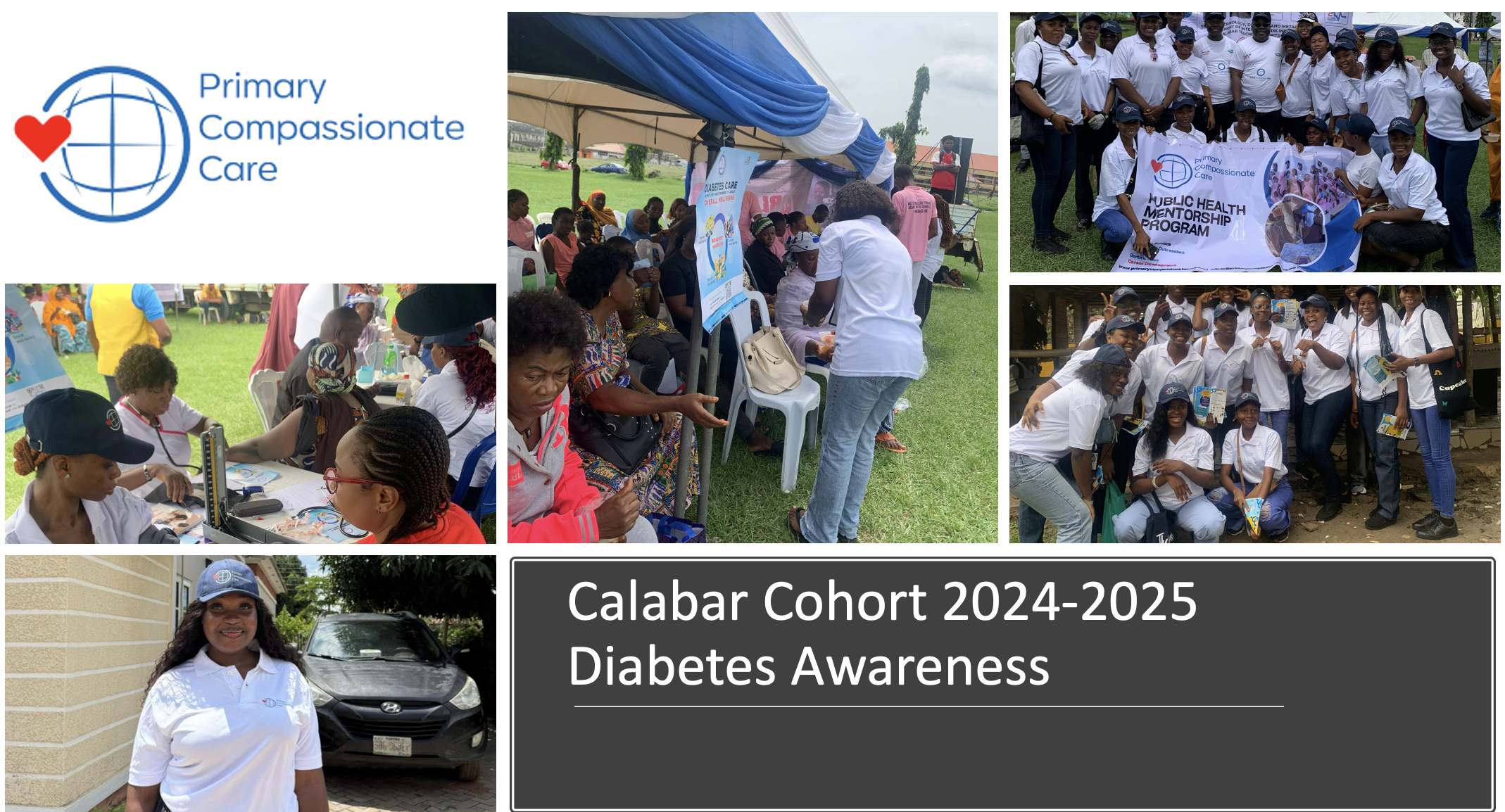
Today, our Primary Compassionate Care team proudly celebrated the graduation of our Calabar Cohort (2024–2025). This milestone marks the completion of an educational journey that explored what it truly means to deliver public health in a community setting. We are grateful for the courage, consistency, and compassion each of you demonstrated throughout the journey and to one another along the way.
Over the past year, this cohort has:
+ Participated in 12 lecture series and 7 international commemorations
+ Conducted a health needs assessment and health awareness campaigns
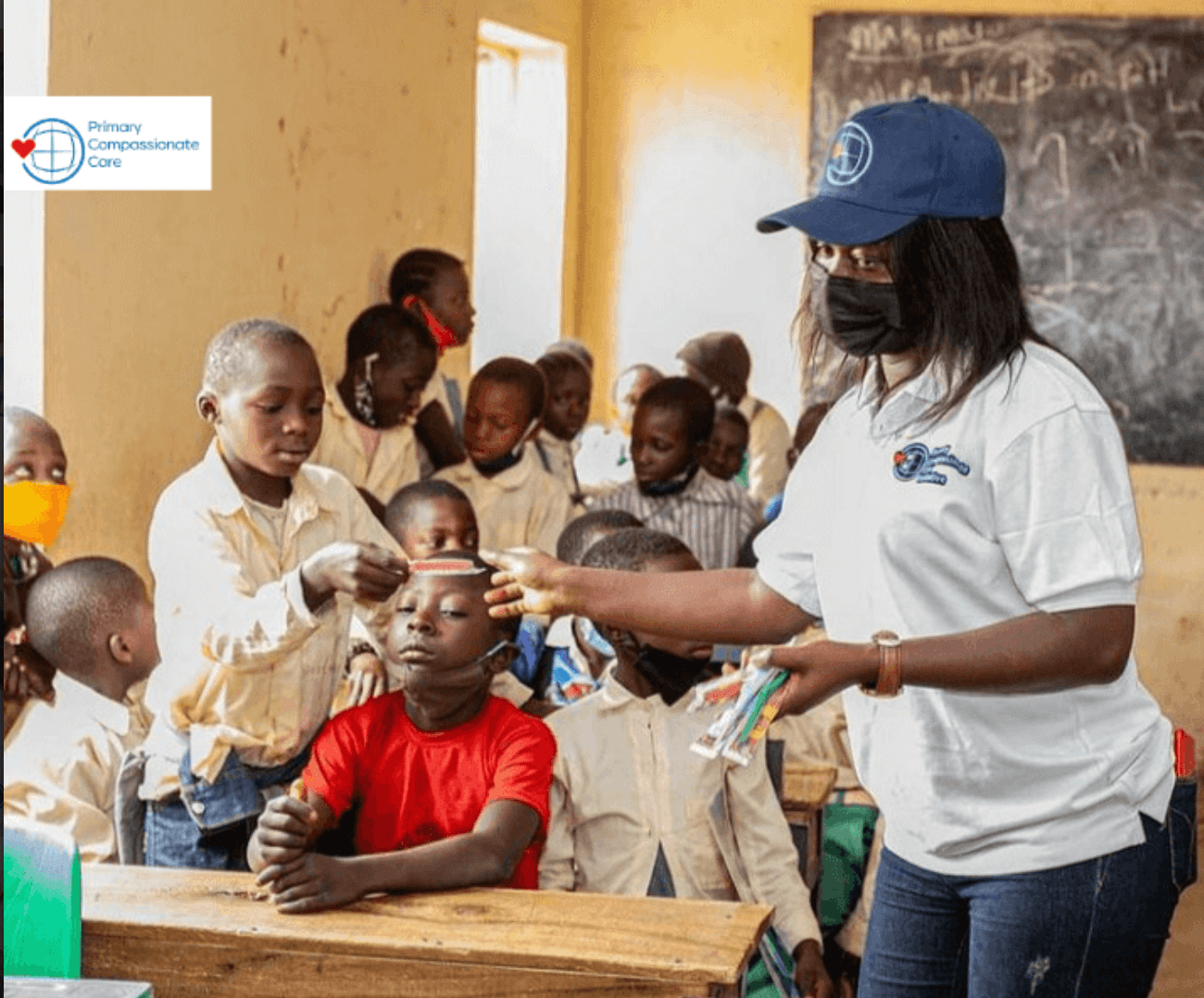
+ Carried out a community intervention project addressing childhood immunization
+ Reached over 1,000 people through advocacy and outreach

Beyond the numbers, what stands out most is the heart behind the work. From creating and launching health campaign videos to educating the public on diabetes awareness, the cohort poured creativity into every effort and demonstrated leadership that inspired others.
🎉 Special congratulations to our awardees:
🏆 Most Participatory: Etimita Oyonnonke Patrick
🏆 Best Team Player: Daniel Blessing Effiong
🏆 Most Socially Engaging: Yojorsam Okoi
To every graduate: Dr. Aisha Liman and I want thank you for dedicating your time and energy to this experience. You proved you can lead, advocate, and inspire through your ability to learn and overcome your own challenges.

We wish you the best!