Under the cherry blossoms
strangers are not
really strangers
Category Archives: Uncategorized
Silence
Spring is leaving
Birds cry, and in the fishes’ eyes
are tears.
~ Chiyo-ni
Bloom!

“How much do we really know about the plants and flowers in our gardens and vases? Beyond their beauty, many have surprising stories of exploration, exchange, and discovery. In Bloom takes visitors from Oxford across the world and back, tracing the journeys that some of Britain’s most familiar blooms travelled to get here. Featuring more than 100 artworks, including beautiful botanical paintings and drawings, historical curiosities and new work by contemporary artists, the exhibition follows the passion and ingenuity of early plant explorers and the networks that influenced science, global trade and consumption. Visitors will learn how plants changed our world and left a legacy that still shapes our environments and back gardens today.” ~ Ashmolean Museum, Bloom Exhibit 2026
Art by Claire Desjardins
AI: Integration & Preparedness

“The General Medical Council (GMC) states that doctors ‘are responsible for the decisions they make when using new technologies like AI, and should work only within their competence.’15 This coincides with the World Medical Association calling for reviewing medical curricula and education for all healthcare stakeholders to improve understanding of the risks and benefits of AI in healthcare.16 It follows then that in fostering good medical practice, medical schools must prepare students for the clinical environment that awaits them through building competence and familiarity in this evolving domain.
With 2 in 3 physicians using AI in their clinical practice, an increase of 78% from 2023,17 enthusiasm for the technology is rapidly growing. Yet, despite this uptake, a 2024 international survey of over 4500 students across 192 medical, dental, and veterinary faculties found that over 75% reported no formal AI education in their curriculum, highlighting a critical gap between technological advancement and medical training.18 This discrepancy underscores the urgency for medical schools to proactively incorporate AI teaching to ensure graduates are ready for the realities of modern clinical practice.”
Read more on Artificial Intelligence in Medical Education: Promise, Pitfalls, and Practical Pathways here.
AI-Enabled Medical School

Succi, Chang, and Rao argue that medical education needs a deliberate redesign for an AI-rich clinical world, not just a bolt-on “AI lecture” or a new tool in the curriculum.
Core argument
- AI, especially large language models (LLMs), is already strong at many clinical-adjacent tasks (documentation, communication support, test-style questions), but performance on benchmarks does not equal genuine clinical reasoning.
- Medical education’s job is to teach reasoning processes and adaptability, not just factual recall or pattern recognition. LLMs can look convincing while still producing plausible but shallow outputs.
Why current LLM success is not the same as clinical reasoning
- The authors emphasize that LLMs often operate via statistical pattern matching, so they can generate confident answers triggered by “buzzwords” or common feature clusters.
- Real clinical reasoning is dynamic: new symptoms appear, data conflict, hypotheses evolve, uncertainty persists. Exams with single best answers do not capture that.
What needs to change in assessment and benchmarking
- They call for new benchmarks that require models to reason step by step through complex cases, justify decisions, and iteratively refine a diagnosis or plan as information changes.
- Validating AI in the education setting, where reasoning can be scrutinized, is presented as a pathway toward trustworthy clinical decision support later.
How AI could reshape teaching and learning
- If LLMs become better at transparent reasoning, they could function as case-based learning partners: tutors, critics of student logic, graders, and discussion counterparts.
- LLMs could help learners at all stages parse difficult materials, including curricula, textbooks, and biomedical literature, which supports lifelong learning in a fast-moving field.
- AI could expand clinical exposure beyond “the patients you happen to see” by generating many varied presentations, including rare diseases and culturally distinct scenarios.
SP-LLMs (standardized patient LLMs)
- The article highlights the idea of LLM-powered standardized patient interactions that can be used for practice and evaluation of communication skills, including exposure to rare and diverse presentations.
Equity and access
- The authors argue LLMs could democratize medical education by distributing expertise at scale, supporting resource-limited settings and schools with lower patient diversity or volume.
- They note that equitable access will require thoughtful licensing models and partnerships between well-resourced and resource-constrained institutions.
What the “AI-enabled physician” must become
- As AI takes on routine tasks, physicians should shift toward higher-level responsibilities: strong clinical reasoning, data interpretation, and ethical oversight of algorithmic outputs.
- Curricula should include “data systems literacy” so future physicians can critically appraise and safely integrate AI outputs into care.
A non-negotiable: dual competency
- The authors stress that technical sophistication must not erode foundational clinical skills. Systems fail, downtime happens, breaches occur, and public health crises arise.
- Training should explicitly reinforce operating both with and without AI, through exercises that require history, exam, and differential diagnosis without digital aids.
Bottom line
Medical schools should integrate AI in ways that strengthen, rather than replace, rigorous reasoning, empathy, and moral judgment. This requires honest engagement with AI limits, new forms of assessment, and collaboration between clinicians, educators, and machine learning experts.
Read more on Building the AI-Enabled Medical School of the Future by Succi, Chang, and Rao.
From Hype to Hospital
Experts from UVic and Island Health discuss safety, evidence, and patient impact of artificial intelligence (AI) in healthcare and research. Learn more and register here.
OpenAI & Health
Purpose of the report
OpenAI’s AI as a Healthcare Ally report explains how ChatGPT and related AI tools are increasingly being used by both patients and healthcare workers to navigate the complex healthcare system, interpret information, and support care decisions. It highlights emerging patterns of use and the potential role of AI as a complement to traditional healthcare rather than a replacement.
Key findings
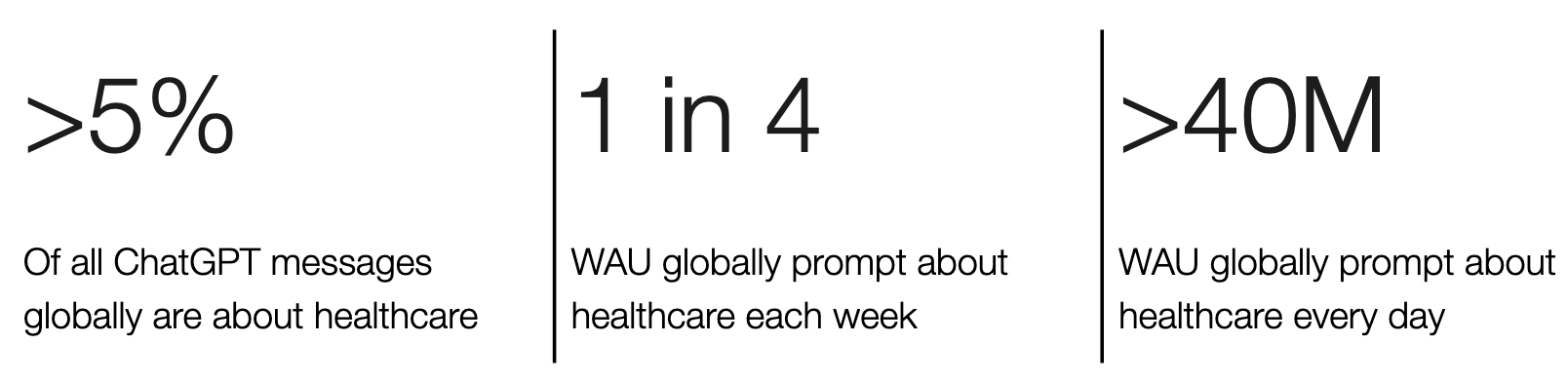
- AI usage for health questions is widespread: over 5% of all ChatGPT interactions globally are health-related; many users ask about symptoms, treatments, medications, insurance, billing and more.
- Millions of people use AI daily: Tens of millions of users (over 40 million globally) consult ChatGPT for health information each day, and roughly one in four users engages with health topics weekly.
- Health queries often occur outside usual clinic hours, reflecting demand when providers are less accessible.
- AI helps with access barriers and complexity: Users in rural or underserved areas use the tool heavily to interpret medical information and navigate administrative tasks such as insurance coverage.
- Clinicians also use AI: Many physicians and nurses report using AI for documentation, admin tasks, and clinical support, suggesting integration into routine practice.
Overall message
The report positions ChatGPT and similar large-language models as informal entry points into healthcare, helping users make sense of medical information, plan care, and reduce complexity. It frames AI as supportive and complementary to clinicians, while acknowledging the need for appropriate safeguards and professional involvement.
If AI can explain your lab results and medication instructions at 11:30 pm, what should “good” use look like, and where should the line be (education vs advice, reassurance vs diagnosis)?
If clinicians are already using AI to help with notes and messages, what do you think should be transparent to patients, and what safeguards would make you feel comfortable?
If millions of people are using AI because the healthcare system is hard to access or hard to navigate, is that a smart workaround, a warning sign, or both?
Share your thoughts in the comment section.
JAMA
Read the most popular JAMA articles in 2025 including coffee and AFib, osteoporosis, platelet transfusion, type 2 diabetes, S aureus bacteremia, septic shock, and more.
Sentiments
“The prudent man always studies seriously and earnestly to understand whatever he professes to understand, and not merely to persuade other people that he understands it; and though his talents may not always be very brilliant, they are always perfectly genuine.
He neither endeavours to impose upon you by the cunning devices of an artful impostor, nor by the arrogant airs of an assuming pedant, nor by the confident assertions of a superficial and imprudent pretender.
He is not ostentatious even of the abilities which he really possesses. His conversation is simple and modest, and he is averse to all the quackish arts by which other people so frequently thrust themselves into public notice and reputation.”
― Adam Smith, The Theory of Moral Sentiments
Deconstructing Adam Smith, 2025
Photography: Jacqueline P. Ashby
Hindsight

In my recent MSc dissertation at the University of Oxford, I explored how medical students experience and perceive artificial intelligence in their learning environment. One thing struck me in their comments: it’s not just AI, it’s the looming feeling of being watched, and not always knowing by whom.
During my integrative literature review, I learned that AI may impact one’s psychological safety as they tended to patients and interacted with colleagues.
As more AI infused tools promise “continuous data” on performance, students described how AI in the hospital setting could become part of their performance evaluation. And not just end of rotation feedback, but a kind of 24/7 visibility. Just the idea of being continuously monitored was enough for students to express that this caused them stress and anxiety.
What stood out to me is that students were not opposed to AI. Many are excited, and eager to learn more about how the technology will be integrated into medicine. What they were asking for was something more basic: transparency, consent, and clear boundaries.
As we adopt AI into medical education, we need to design and integrate for psychological safety. Otherwise, we risk teaching the next generation of physicians to perform for the system, rather than to think with and for their patients. It reminds me of Mayo’s Hawthorne effect and the potential for AI use as a surveillance tool and form of manipulation to boost productivity.
Over the next while I’ll be sharing a few short reflections from this research, paired with my own photography, as a way to keep this conversation human, creative, and thoughtful.
In hindsight, 2025
Photographer: Jacqueline P. Ashby
Kelvingrove Art Gallery and Museum
